


What is a Virtual Medical Scribe? How It Works & Use Cases
Michelle researched virtual medical scribe services across real-time and asynchronous models, breaking down US-based versus offshore pricing, HIPAA compliance, and EHR integration.


A virtual medical scribe is a remote professional who listens to patient encounters (usually in real time) and documents them into the Electronic Health Record (EHR).
They function just like an in-person scribe, but they work from a remote location, often using secure software that allows them to hear or view the consultation through audio or video.
Virtual scribes are trained in medical terminology, documentation styles, and clinical workflows. Their job is to reduce the documentation burden on physicians by taking detailed, accurate notes during or shortly after a visit.
How Does a Virtual Scribe Work?
A virtual scribe works remotely by connecting to the physician’s exam room through a secure audio or video feed. During the consultation, they listen to the interaction and enter notes directly into the Electronic Health Record (EHR), either in real time or shortly after the visit.
Depending on the setup, the scribe may have full or partial access to the EHR, allowing them to assist with note-taking, documentation templates, or even billing codes.
There are two common ways virtual scribing is done:
1. Real-Time Scribing
In this model, the scribe listens to the patient visit live through a secure audio or video connection. They document the encounter in real time as the physician and patient talk.
This ensures that the clinical note is ready for review and sign-off immediately after the visit, which significantly speeds up documentation workflows.
2. Delayed or Asynchronous Scribing
Here, the patient visit is recorded (always with prior consent) and the scribe accesses the recording later to complete the documentation.
While not live, this model still delivers accurate, high-quality notes and is often preferred in clinics where real-time internet connections are inconsistent or where physicians want flexibility in how documentation support is provided.
In both models, the virtual scribe follows the provider’s preferred documentation style and ensures that clinical notes meet compliance and billing standards.
{{templates}}
5 Reasons Why You Need a Virtual Medical Scribe
1. More Time for Patient Care
With a virtual scribe handling the EHR, physicians can maintain eye contact and engage more naturally with patients instead of typing notes. This improves the overall experience for both doctor and patient, helping build stronger communication and trust during each visit.
2. Lower Risk of Burnout
Many physicians report spending one to two hours on documentation for every hour they spend seeing patients. Over time, this leads to late nights, fatigue, and burnout. Virtual scribes reduce this load by completing documentation during or immediately after the visit, freeing physicians from hours of after-work charting.
3. Faster and More Accurate Charting
Virtual scribes document the visit in real time or soon after, which means charts are completed faster and with better accuracy. Physicians no longer need to rely on memory to fill in details later, and billing processes can begin sooner thanks to timely documentation.
4. More Cost-Effective Than In-Person Scribes
Hiring an in-person scribe often involves training, office space, and administrative overhead. Virtual scribes eliminate these extra costs while still delivering the same benefits. For many practices, this remote setup offers a more budget-friendly way to reduce documentation work without compromising quality.
5. Scalable for Multi-Location and Telehealth Practices
Whether you're expanding your clinic, managing multiple locations, or offering telemedicine, virtual scribes provide a scalable solution. Since they work remotely, a single scribe can support different providers or shifts across time zones, making them highly flexible for growing or distributed healthcare teams.
What is the Difference Between a Virtual Scribe and an AI Scribe?
Virtual scribes offer more accuracy and flexibility, while AI scribes are cheaper and better for high-volume routine tasks.
Here’s a quick overview of the two:
Some providers use hybrid models, where an AI drafts the note and a human reviews or edits it.
How to Choose a Virtual Medical Scribe Service
Not all virtual scribe services are the same. Choosing the right one can make the difference between smooth, accurate documentation and daily frustration.
Here’s what to look for before you commit:
1. Scribe Training and Experience
Ask how the company trains its scribes. Do they understand medical terminology, SOAP note formats, and your specialty’s unique requirements? An experienced scribe will adapt quickly and deliver notes that match your workflow with minimal corrections.
2. Specialty-Specific Support
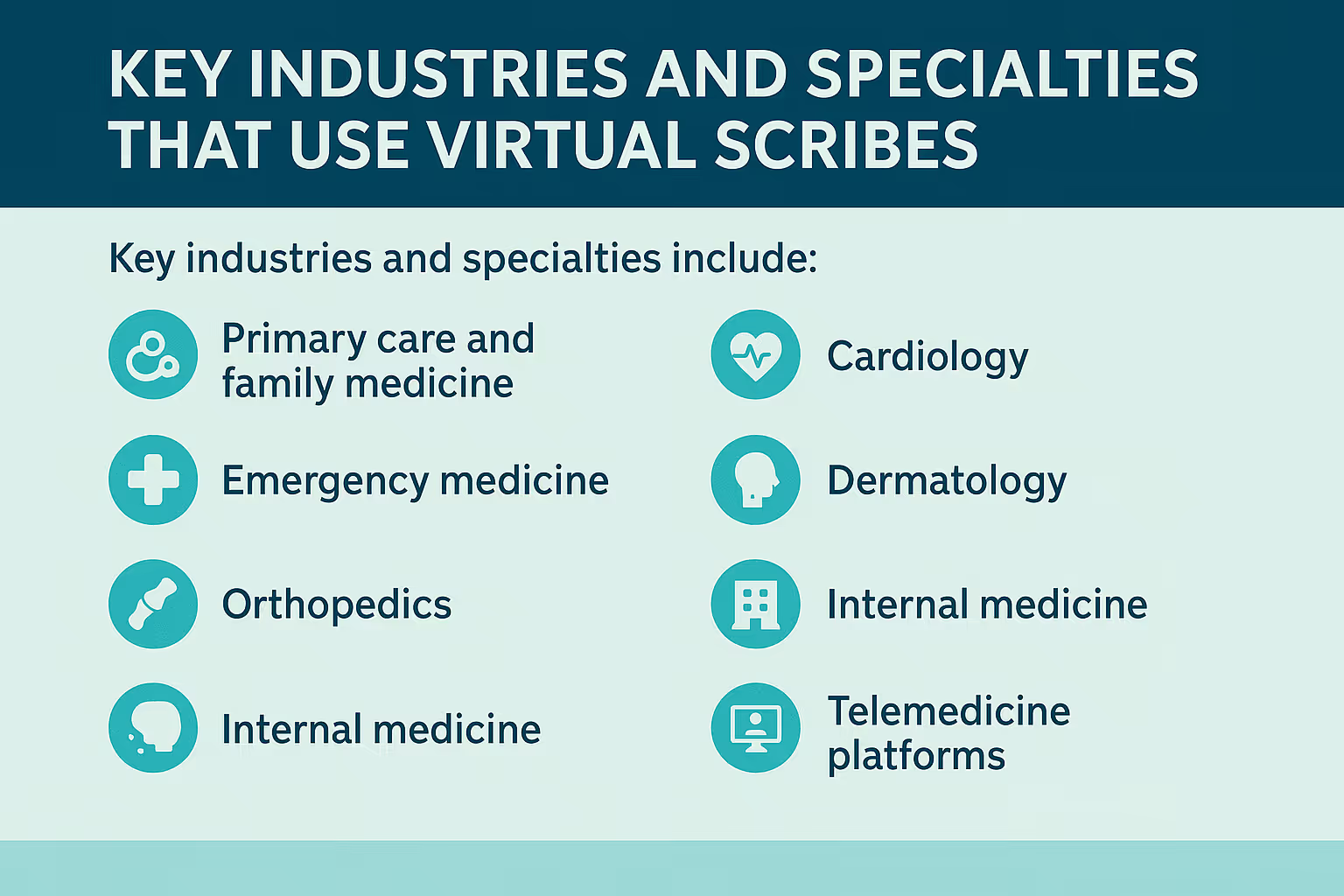
Many services only offer general documentation. If you work in a specialized field like cardiology, dermatology, or orthopedics, you need scribes who understand that domain. Look for providers that can match you with scribes trained in your area of care.
3. Live vs. Asynchronous Scribing Options
Decide whether you prefer real-time documentation during the visit or post-visit transcription based on recordings. Real-time scribing helps you complete notes immediately, while asynchronous models offer flexibility if your internet setup is limited.
4. EHR Compatibility
Make sure the scribe service integrates well with your Electronic Health Record system. Some scribes document directly inside your EHR, while others may send drafts for manual entry. The smoother the integration, the more time you’ll save.
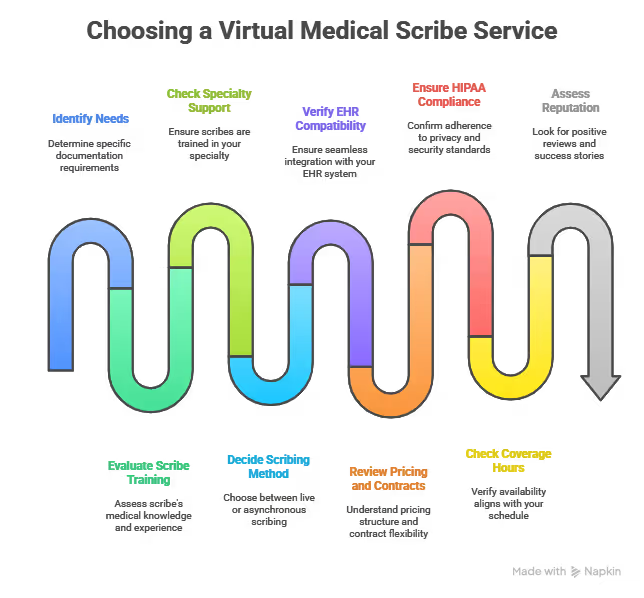
5. Transparent Pricing and Flexible Contracts
Review the pricing structure carefully. Some vendors charge flat monthly rates; others bill hourly. Also, check the terms: are you locked into long contracts, or can you scale up or down easily as your needs change?
6. HIPAA Compliance and Data Security
Your scribe will be handling sensitive patient data, so the service must meet strict privacy standards. Ask about HIPAA compliance, encryption protocols, and whether they’re willing to sign a Business Associate Agreement (BAA).
7. Coverage Hours and Availability
Consider when you need support. Do you see patients during weekends or evenings? Some services only provide weekday coverage, while others offer 24/7 availability. Make sure their hours match your clinic schedule.
8. Reputation and Proof of Results
Look for case studies, client reviews, or references. A good scribe service should have documented success stories that show how they’ve improved workflow, saved time, or reduced charting backlog for other providers.
{{cta}}
How Much Does a Medical Scribe Cost?
If you’re thinking about hiring a virtual scribe, you should know the cost depends on a few key factors.
These include how many hours you need coverage, the complexity of your specialty, whether you want real-time support or delayed transcription, and whether the scribe is based in the US or offshore.
Here’s what you can expect to pay:
US-based scribes usually cost more because of higher wages and stricter compliance standards, but they also tend to offer better contextual accuracy.
Offshore scribes offer a more affordable option for practices with budget constraints. If you want to lower costs even further, consider AI-assisted scribes that combine automation with human review.
Make sure to choose a model that fits your workflow, documentation needs, and budget, without compromising on quality or patient experience.
Virtual Medical Scribe Risks and Challenges (And How AI Helps)
While virtual scribes offer major efficiency gains, there are also some real challenges to consider. Understanding these risks helps you make better decisions, and AI-powered tools like Lindy can often solve or minimize many of these problems.
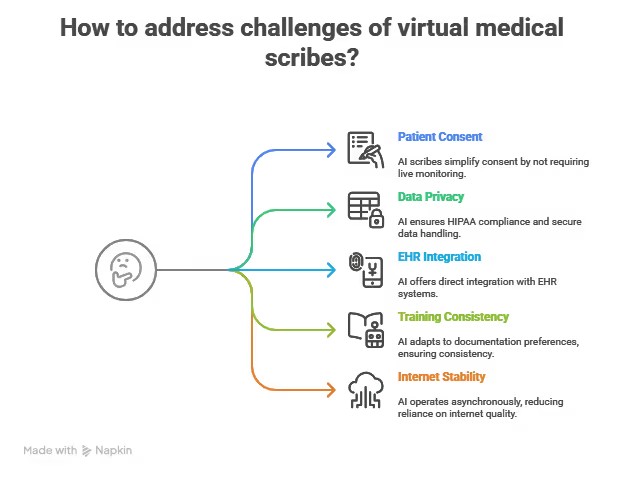
1. Patient Consent Is Required
Any time a scribe joins remotely or a consultation is recorded, you must inform the patient and get explicit consent. This is a legal and ethical requirement that can slow down onboarding or introduce friction in care.
AI scribes like Lindy don’t require a live human listening in, which simplifies the consent process. Since the tool works locally or with structured data input, patients often feel more comfortable knowing no third party is monitoring the visit. However, you should always check your local regulations and organizational policies regarding patient consent.
2. Strict Data Privacy and HIPAA Compliance
Your scribe provider handles sensitive health information. If they’re not fully HIPAA-compliant, your practice risks legal action, fines, and loss of trust. It’s also essential to ensure secure data transmission and storage.
Lindy is built with enterprise-grade data security and offers HIPAA compliance, end-to-end encryption, and local data controls. You can review access logs, set permissions, and sign a Business Associate Agreement (BAA) to stay fully compliant.
3. EHR Integration Can Be Complex
Some scribe services don’t integrate directly with your EHR, requiring manual copy-paste or review workflows. This increases time, reduces accuracy, and slows adoption by your team.
Lindy supports direct integration with major EHR systems through secure APIs. You can also use Lindy to automate documentation tasks, generate structured notes, and sync them back into your patient records, without disrupting your existing workflow.
4. Training and Consistency Issues
Every provider documents differently. Virtual scribes often need time to learn your style, and inconsistency across scribe teams can lead to errors or rework. This is especially common with outsourced or offshore teams.
Lindy adapts to your documentation preferences using fine-tuned templates and custom prompts. Over time, it learns your style and automatically applies consistent formatting, phrasing, and coding logic– no retraining or reassignments needed.
5. Reliance on Internet Stability
Real-time scribing requires a stable, high-quality internet connection. If your bandwidth is limited or your clinic has network issues, you may face delays, dropped sessions, or lost data.
Lindy does not rely on live streaming or external connections during the visit. It works asynchronously and can operate from transcripts, audio uploads, or structured inputs. This removes dependence on real-time internet quality and keeps workflows stable even in low-bandwidth environments.
Why It’s Better to Automate Medical Documentation
Automating your clinical documentation offers more than just convenience; it directly improves efficiency, accuracy, and your quality of life as a provider.
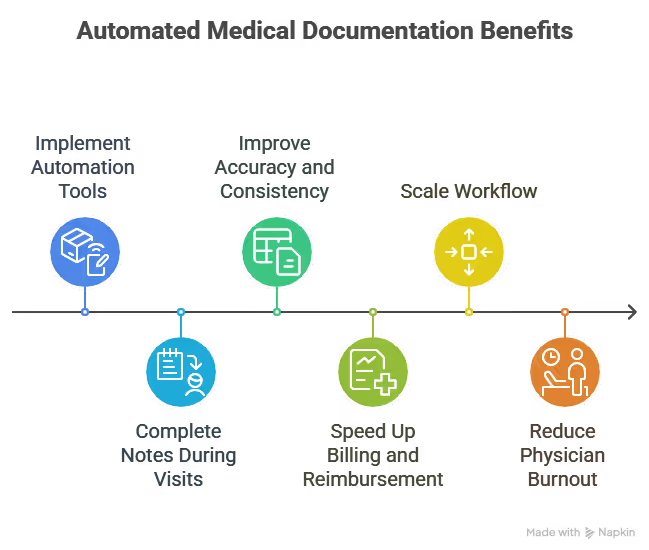
Here’s how:
1. Save Time During and After Visits
When you automate documentation with a virtual scribe or AI tool, your notes get completed as the visit happens or shortly after. You no longer need to stay late finishing charts or spend weekends catching up. This gives you more time to see patients, take breaks between appointments, or simply finish work on time.
2. Improve Accuracy and Consistency
Automated documentation tools follow structured templates and listen to the full patient conversation. That means fewer missed details, clearer histories, and more complete exam notes. Over time, this improves the quality of your records and ensures every chart reflects the actual care provided, especially helpful for billing, audits, and legal protection.
3. Speed Up Billing and Reimbursement
With complete and accurate notes available immediately, your billing team can submit claims faster. There’s less back-and-forth for clarification and fewer denials from incomplete documentation. This improves your cash flow and helps your practice run more smoothly.
4. Scale Your Workflow Without Hiring More Staff
As your practice grows, automation helps you keep up without needing to hire additional administrative support. Whether you’re expanding to more locations or adding telehealth, a virtual or AI scribe setup can scale with you, covering more hours and more providers with minimal overhead.
5. Reduce Physician Burnout
Documentation is one of the biggest causes of physician stress. Automating this task lets you focus on patient care and meaningful conversations, not on remembering symptoms or typing up long notes. When your mental load is lighter, you deliver better care and protect your own well-being.
Ready to Automate Medical Documentation the Smart Way?
If you’re tired of juggling patient care with endless charting, now is the time to shift toward intelligent automation.
Lindy gives you the power of an AI scribe without the complexity of traditional remote setups. It’s faster than manual documentation, more scalable than hiring new staff, and built to meet the real-world needs of modern healthcare teams.
With Lindy, you can:
- Capture notes automatically from voice, transcripts, or text
- Customize output to match your documentation style and specialty
- Integrate directly with your EHR for seamless chart updates
- Stay HIPAA-compliant with secure encryption and BAA support
- Save hours per week while improving billing speed and accuracy
Frequently Asked Questions
1. Can a medical scribe work from home?
Yes, many medical scribes work remotely. They connect to the exam room using secure audio or video tools and document the visit in real time or after it ends. This setup allows them to support multiple providers without being physically present in the clinic.
2. How does a medical scribe help a physician?
A medical scribe handles documentation during patient visits. This allows physicians to focus more on patients and less on typing notes. Scribes capture histories, exam findings, and treatment plans, reducing after-hours charting and helping doctors work more efficiently during the day.
3. How does virtual scribing work?
Virtual scribes connect to live or recorded patient visits using secure technology. They listen to the conversation and enter notes into the electronic health record. Depending on the setup, they may work in real time or complete the documentation after reviewing recordings.
4. How to hire a scribe?
You can hire a scribe through a staffing agency, a virtual scribe service, or by recruiting directly. Look for candidates with strong medical knowledge and EHR experience. Interview them, check references, and ensure they understand your specialty and documentation style.
5. Is Happy Scribe legit?
Yes, Happy Scribe is a legitimate transcription tool. It provides audio-to-text services for general content but is not designed for clinical documentation. It works well for interviews, lectures, and media, but does not replace medical scribes or AI scribe platforms built for healthcare.
6. Is ScribeAmerica legit?
Yes, ScribeAmerica is a reputable company that provides in-person and virtual medical scribes to clinics and hospitals. It has worked with thousands of healthcare providers and offers training, support, and staffing services across multiple specialties and care settings.
7. Is Scribe free?
No, medical scribe services are not free. Whether you use a human scribe or an AI tool, you need to pay a monthly or per-hour fee. Costs vary based on features, specialty support, real-time access, and whether the service is based in the US or offshore.
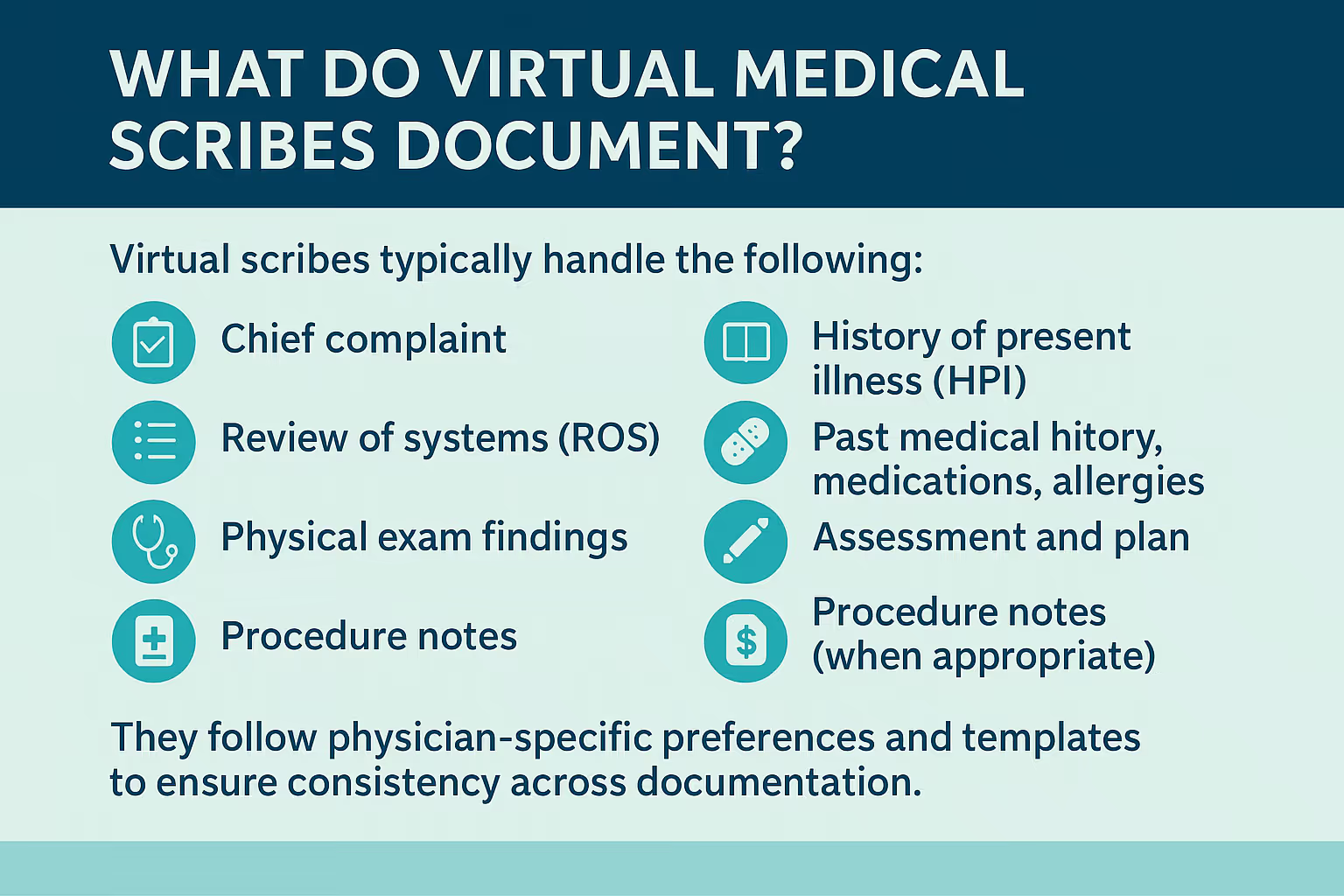
8. What do medical scribes do?
Medical scribes document patient encounters for physicians. They write histories, physical exam findings, and treatment plans. Scribes also help organize notes, track time-sensitive tasks, and improve EHR accuracy. Their role helps doctors stay focused on patient care instead of typing and navigating software.
9. What does a telescribe do?
A telescribe works remotely to support a physician during patient visits. They join through audio or video connections and handle real-time or delayed documentation. Telescribes help reduce charting workload, improve efficiency, and support clinics that cannot accommodate on-site scribes.
10. How much does DeepScribe cost?
DeepScribe pricing varies depending on practice size, note volume, and integration needs. Plans typically start around $500 per month per provider and can go higher with premium features. You should contact the company directly to get a custom quote based on your setup.
11. Is a virtual scribe HIPAA-compliant?
Yes, if the vendor uses secure systems and signs a Business Associate Agreement. You should confirm their encryption methods, access controls, and compliance certifications before sharing patient data. HIPAA compliance protects your practice from legal and financial risk.
12. Do patients need to consent for a virtual scribe?
Yes, you must tell patients that a virtual scribe will hear or record the visit. Most services offer consent templates you can use. Getting clear permission ensures compliance with privacy laws and builds trust between you and your patients.
13. Can a virtual scribe enter data directly into my EHR?
Yes, many virtual scribes have permission to document directly inside your EHR. Others use secure portals or transcription software that integrates with your system. Always verify their access level, experience with your EHR, and compatibility before starting.
14. How do virtual scribes handle different specialties?
Virtual scribe companies train staff in various specialties like cardiology, dermatology, or emergency medicine. They learn relevant terminology and documentation formats. When hiring, ask if the scribe has experience in your field to ensure accurate and efficient note-taking.
15. What’s better: AI or human scribes?
It depends on your needs. Human scribes provide higher accuracy and adapt well to complex cases. AI scribes work faster and cost less. Many clinics use a hybrid model where AI drafts the notes and a human reviews or edits them before finalizing.














Blog
Related Articles
.png)

.png)
%20(1).png)
.avif)

%20(1).png)
.png)
The AI assistant that runs your work life
Lindy saves you two hours a day by proactively managing your inbox, meetings, and calendar, so you can focus on what actually matters.
